Discrete Trial Training (DTT) is a structured ABA teaching method that breaks complex skills into small, repeatable steps. Each step follows a clear pattern: an instruction, your child’s response, and a reward for the correct answer. DTT is most effective for children ages 2 to 7 and is delivered by trained therapists in sessions of 1 to 3 hours.
If your child has just started Applied Behavior Analysis (ABA) therapy or you are considering it, you have likely heard the term Discrete Trial Training. It is one of the most studied teaching methods in autism intervention, and it is almost certainly part of your child’s program in some form.
This guide explains what DTT is, exactly how it works, what a session looks like, and how the modern version differs from the older 1980s approach you may have read about online.
What is Discrete Trial Training in ABA Therapy?
Discrete Trial Training is a teaching method within ABA that breaks down skills, such as naming colors, requesting items, or making eye contact, into the smallest possible learning units called trials. Each trial is short, structured, and repeated until the child masters the skill before moving on to the next one.
The method was developed in the 1970s and refined through the 1980s by Dr. O. Ivar Lovaas at the University of California, Los Angeles (UCLA). His 1987 study, published in the Journal of Consulting and Clinical Psychology, became one of the most influential autism intervention studies in history [1].
Three things make DTT different from regular teaching:
- It is highly structured. Every trial follows the same pattern, which creates predictability for children who thrive on routine.
- It is data-driven. Therapists record whether each trial was correct, incorrect, or required a prompt, so progress is measurable.
- It uses positive reinforcement. Correct responses are immediately rewarded with praise, a small treat, or a preferred item or activity.
DTT is not a separate therapy from ABA. It is one technique within ABA, and modern programs combine it with naturalistic methods such as Natural Environment Teaching (NET) and Pivotal Response Treatment (PRT) [2].
Not sure if ABA therapy is the right step for your child?
Get our free 5-minute parent checklist — the same questions our BCBAs use during intake to assess fit.
How Does DTT Work? Inside Every Trial
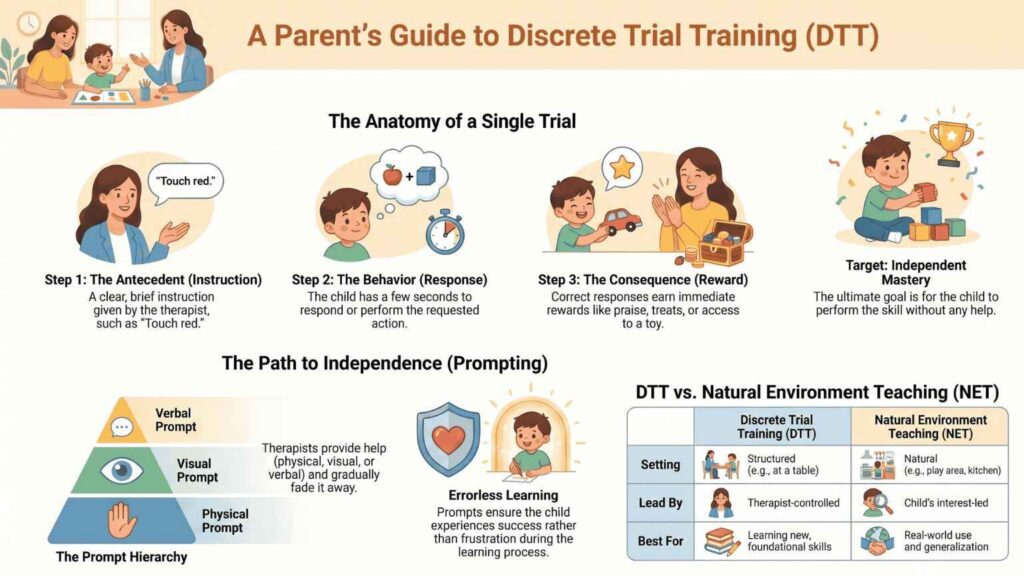
Every discrete trial has the same five parts: the antecedent, the prompt, the response, the consequence, and the inter-trial interval. Therapists often shorten this to the ABCs of ABA Antecedent, Behavior, Consequence because the prompt and interval are smaller supporting pieces.
1. Antecedent (the instruction)
The therapist gives a clear, brief instruction called the discriminative stimulus, or SD. The instruction is short, specific, and given only once per trial. Examples of antecedents include “Touch your nose,” “What color is this?”, or holding up two cards and saying “Find the apple.”
2. Behavior (your child’s response)
After the antecedent, your child has a few seconds to respond. The response is the behavior the therapist is trying to teach: pointing at the apple, saying “red,” touching their nose. If your child responds correctly, the trial moves to the consequence. If not, the therapist provides a prompt and tries again.
3. Consequence (the reinforcement)
A correct response earns immediate positive reinforcement, such as enthusiastic praise, a small piece of a favorite snack, a token toward a larger reward, or 10 to 15 seconds of access to a preferred toy. An incorrect response receives a calm, neutral correction not frustration or punishment and the trial is repeated with more support [3].
4. The Inter-Trial Interval
Between trials, the therapist pauses briefly (1 to 5 seconds), records the data, and then starts the next trial. This short pause helps your child reset before the next instruction.
Did You Know?
A single trial usually lasts 5 to 20 seconds. A 1-hour DTT session might contain 100 or more trials, although modern programs often mix DTT with play-based teaching rather than running back-to-back trials for the full hour.
What Does a DTT Session Look Like?
A typical DTT session lasts 1 to 3 hours and takes place in one of three settings: your home, a therapy center, or your child’s school. The therapist is usually a Registered Behavior Technician (RBT) working under the supervision of a Board Certified Behavior Analyst (BCBA) [4].
Here is what a real session might look like for a 4-year-old child working on color identification:
- The therapist sets up at a small table with two colored cards (red and blue) and a small bin of preferred toys nearby.
- The therapist says, “Touch red” (antecedent).
- The child touches the red card (behavior).
- The therapist says, “Great job!” and lets the child play with a favorite toy car for 10 seconds (consequence).
- After the play break, the therapist resets the cards and runs the next trial.
Over the session, the therapist will mix in trials for other skills the child is working on, perhaps imitating a clap, answering “What’s your name?”, or following a one-step direction. This rotation prevents boredom and helps the child generalize skills across contexts.
What Skills Can DTT Teach My Child?
DTT works best for skills that can be broken into clear, observable steps. Skills commonly taught with DTT include receptive language (following instructions), expressive language (labeling objects, answering questions), imitation (copying movements or sounds), academic readiness (matching, sorting, counting), and self-help skills (handwashing steps, dressing steps).
DTT is less effective for skills that depend on spontaneity, creativity, or unstructured social interaction. Those skills are better taught through naturalistic methods such as NET or PRT. This is why most modern ABA programs use DTT alongside other techniques rather than relying on it alone [5].
Wondering which skills your child would work on first?
How Prompts And The Prompt Hierarchy Work in DTT
A prompt is any help the therapist gives your child to produce the correct response. Prompts are used so the child experiences success and gets reinforced, rather than failing repeatedly. The goal is to fade prompts over time until the child can respond independently.
Therapists use a prompt hierarchy that moves from most to least supportive:
- Full physical prompt: the therapist physically guides your child’s hand to complete the response.
- Partial physical prompt: the therapist gently nudges the child’s elbow or wrist toward the correct answer.
- Model prompt: the therapist demonstrates the response and the child copies it.
- Gestural prompt: the therapist points to or looks at the correct answer.
- Verbal prompt: the therapist gives a hint, such as the first sound of the word.
- Independent: no prompt needed. This is the goal.
Most BCBA-designed programs use either most-to-least prompting (start with strong support and fade) or least-to-most prompting (start with no support and add more if needed), depending on your child’s learning history.
Is DTT Outdated or Still Used in Modern ABA?
This is one of the most common questions parents ask, and the honest answer is: modern DTT is very different from 1980s DTT, but the underlying method is still used and still works.
The original Lovaas program used 40 hours per week of one-on-one DTT, often delivered at a table for long stretches, with aversive consequences sometimes used for incorrect responses [1]. Modern ABA has moved away from rigid table-only DTT and away from any form of aversive consequence. Today’s DTT is shorter, blended with naturalistic teaching, child-led whenever possible, and exclusively positive-reinforcement-based [6].
Research evidence remains strong. A 2009 systematic review published in Research in Autism Spectrum Disorders found that Early Intensive Behavioral Intervention (EIBI), which uses DTT as a core component, produced significant gains in IQ, adaptive behavior, and language skills compared to control groups [7]. The American Academy of Pediatrics continues to recognize ABA-based interventions as evidence-based for autism spectrum disorder [8].
The phrase you may hear from your BCBA is “evidence-based but evolved.” DTT is still in the toolkit. It is no longer the only tool.
DTT vs Natural Environment Teaching (NET): How They Work Together
DTT and NET are often described as opposites, but a well-designed ABA program uses both. The difference lies in who leads the learning and where it happens.
Feature | Discrete Trial Training (DTT) | Natural Environment Teaching (NET) |
Setting | Table, structured area | Wherever the child is floor, kitchen, playground |
Who leads | Therapist | Child’s interest |
Pace | Therapist-controlled | Child-controlled |
Reinforcer | Often unrelated to task (e.g., a toy for naming colors) | Naturally related to task (asking for juice → getting juice) |
Best for | New skill acquisition, foundational skills | Generalization, spontaneous communication |
A typical session for a young child might start with 20 minutes of DTT at a table (to build a new skill), followed by 30 minutes of NET on the floor (to help the child use that skill in real play), followed by another short DTT block.
e cover NET in depth in our guide to Natural Environment Teaching, and for a complete comparison of all four major ABA methods, including when each fits a child best, see our guide to Types of ABA Therapy Methods: DTT, NET, PRT, and VB Explained.
Ready to talk to a BCBA about your child?
Frequently asked questions about DTT
Is DTT safe for my child?
Yes. Modern DTT uses only positive reinforcement and removes any form of punishment. The structured format actually reduces anxiety for many children with autism, because the predictability of trials creates a sense of safety.
At what age does DTT work best?
Research consistently shows the strongest outcomes when ABA-based intervention, including DTT, begins between ages 2 and 5 [7]. DTT is still effective for older children and teens, but the learning curve is faster in the early years.
How many hours per week of DTT does my child need?
There is no single number that fits every child. Comprehensive ABA programs range from 25 to 40 hours per week, with DTT making up only part of that time. Focused programs may run 10 to 20 hours per week. Your BCBA will recommend an intensity based on your child’s assessment and goals. See our guide on Focused vs Comprehensive ABA for more detail.
Can I do DTT with my child at home, without a therapist?
Parents can absolutely support DTT-style learning at home, and we encourage it. However, full DTT programming should be designed and supervised by a BCBA to ensure correct prompting, reinforcement timing, and data collection. Our parent training program teaches caregivers the techniques that support carryover at home.
Does insurance cover DTT-based ABA?
Yes. DTT is considered part of standard ABA therapy, which is covered by most major insurance plans including Aetna, Cigna, UnitedHealthcare, Anthem BCBS, and Medicaid in eligible states. See our ABA therapy insurance guide for New York for details on coverage and how to verify your benefits.
Talk to a BCBA about whether DTT fits your child
Every child responds differently to teaching methods. The right approach for your child depends on their age, current skills, learning style, and goals and that requires a proper assessment by a Board Certified Behavior Analyst. Our team has supported families across New York, New Jersey, Connecticut, Georgia, and North Carolina since 2015 and would be glad to answer your questions.
References
[1] Lovaas, O. I. (1987). “Behavioral treatment and normal educational and intellectual functioning in young autistic children.” Journal of Consulting and Clinical Psychology, 55(1), 3–9.
https://pubmed.ncbi.nlm.nih.gov/3571656/
[2] Smith, T. (2001). “Discrete Trial Training in the Treatment of Autism.” Focus on Autism and Other Developmental Disabilities, 16(2), 86–92.
https://journals.sagepub.com/doi/10.1177/108835760101600204
[3] Indiana Resource Center for Autism, Indiana University Bloomington. “Discrete Trial Teaching: What Is It?”
https://iidc.indiana.edu/irca/articles/discrete-trial-teaching-what-is-it.html
[4] Behavior Analyst Certification Board (BACB). “About Behavior Analysis: BCBA and RBT roles.”
https://www.bacb.com/about-behavior-analysis/
[5] Association for Science in Autism Treatment (ASAT). “UCLA/Lovaas Intervention.”
https://asatonline.org/for-parents/learn-more-about-specific-treatments/applied-behavior-analysis-aba/aba-techniques/uclalovaas-intervention/
[6] McEachin, J. J., Smith, T., & Lovaas, O. I. (1993). “Long-term outcome for children with autism who received early intensive behavioral treatment.” American Journal on Mental Retardation, 97(4), 359–372.
https://pubmed.ncbi.nlm.nih.gov/8427693/
[7] Reichow, B., & Wolery, M. (2009). “Comprehensive synthesis of early intensive behavioral interventions for young children with autism based on the UCLA Young Autism Project model.” Journal of Autism and Developmental Disorders, 39(1), 23–41.
https://pubmed.ncbi.nlm.nih.gov/18535894/
[8] Hyman, S. L., Levy, S. E., Myers, S. M., & AAP Council on Children with Disabilities. (2020). “Identification, Evaluation, and Management of Children With Autism Spectrum Disorder.” Pediatrics, 145(1).
https://publications.aap.org/pediatrics/article/145/1/e20193447/36917/
