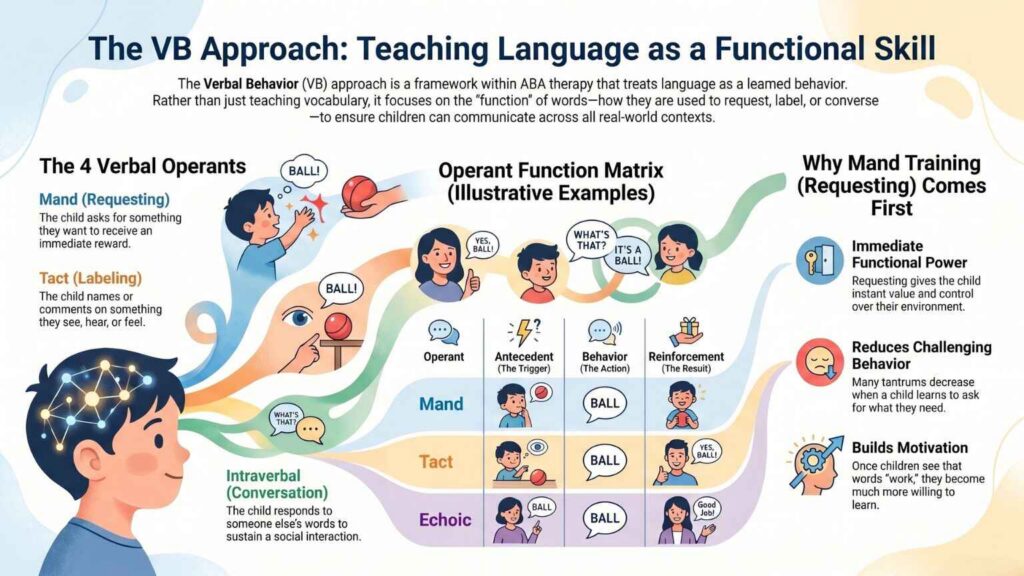
The Verbal Behavior (VB) Approach teaches language within ABA therapy by treating it as functional behavior. Based on B.F. Skinner’s analysis, VB therapy targets four verbal operants: mand (requesting), tact (labeling), echoic (repeating), and intraverbal (conversation).
If your child is in ABA therapy and you’ve heard terms like mand or VB-MAPP during meetings with your BCBA, you’re already inside a Verbal Behavior program. The VB approach is one of the most influential frameworks in modern ABA, especially for children with autism who are learning to communicate.
This guide explains what the VB approach is, the four verbal operants in plain language, why mand training comes first, and how VB fits alongside other ABA methods like DTT, NET, and PRT.
What is the Verbal Behavior (VB) Approach in ABA?
The Verbal Behavior approach is a framework within ABA therapy that teaches language by focusing on its function rather than its form. Instead of teaching a child what a word means and assuming they can use it in every context, VB therapy teaches each different use of language as a separate skill.
The approach is built on B.F. Skinner’s 1957 book Verbal Behavior, in which he proposed that language is a learned behavior governed by the same principles as any other behavior, antecedent, behavior, and reinforcement [1]. Skinner argued that knowing a word in one context does not automatically mean a person can use that word in every other context. Decades of research have confirmed this, especially in children with autism.
The VB approach was developed into a practical therapy framework in the 1980s and 1990s by behavior analysts Jack Michael, Mark Sundberg, Jim Partington, and Vince Carbone [2]. Today, it is a standard part of modern ABA therapy and the foundation of the widely used VB-MAPP assessment tool [3].
Three things define the VB approach:
- Language is treated as behavior, governed by motivation and reinforcement just like any other learned skill.
- Each verbal function is taught separately until the child can use the same word across different functions.
- Mand training (requesting) is prioritized first, because it gives communication immediate value to the child.
Looking for ABA therapy that builds real communication, not just vocabulary?
Tell us about your child and our BCBA team will reach out to discuss how a VB-based ABA program at ABS could support your child’s language development.
How is VB Different From Traditional Speech Therapy?
Speech therapy and the VB approach both teach communication, but they approach it from different angles.
Traditional speech therapy typically focuses on the form of language articulation, vocabulary size, grammar, and pronunciation. A speech therapist might work on helping a child say the “r” sound correctly, or expand their vocabulary from 20 words to 100.
The VB approach focuses on the function of language, what the child can do with the words they have. A VB program might focus less on adding new words and more on ensuring the child can use the words they already know in every meaningful way: to request, to label, to repeat, and to converse [4].
Both approaches are valuable, and many children with autism receive both VB-based ABA therapy and traditional speech therapy. They complement each other rather than compete. Your child’s BCBA and Speech-Language Pathologist (SLP) will typically coordinate goals so the two programs reinforce each other.
For a deeper comparison of the methods used in ABA, see our guide on ABA therapy techniques for speech.
What Are The 4 Verbal Operants?
The VB approach teaches that there are four primary verbal operants, different functions a single word can serve [5]. The same word, “ball,” can function as four different verbal operants depending on context. Here is what each operant means and what it looks like in real life:
1. Mand (Requesting)
A mand is a request. The child says a word because they want something. The reward for a successful mand is getting the thing they asked for.
- Antecedent: The child wants something (this is called a “motivating operation”)
- Behavior: The child says “ball”
- Reinforcement: The child gets the ball
Mands are arguably the most important verbal operant because they give the child immediate, functional power over their environment. A child who can mand can ask for what they need instead of crying, screaming, or grabbing.
2. Tact (Labeling or Commenting)
A tact is a label or comment about something the child sees, hears, feels, or experiences.
- Antecedent: The child sees a ball roll across the floor
- Behavior: The child says “ball”
- Reinforcement: Social attention, such as the parent saying “Yes! That’s a ball!”
Tacts let the child share their experience of the world with others. Many children with autism develop strong tact skills (they can label hundreds of objects) without developing strong mand skills (they can’t ask for those same objects).
3. Echoic (Repeating)
An echoic is when the child repeats what someone else just said. The repeated word matches the original word sound-for-sound.
- Antecedent: The therapist says “Say ball”
- Behavior: The child says “ball”
- Reinforcement: Praise from the therapist
Echoic skills are foundational. They make it possible to teach new words because the child can copy what they hear.
4. Intraverbal (Conversation)
An intraverbal is a verbal response to someone else’s words, where the response doesn’t sound exactly like the question. This is a conversation.
- Antecedent: A friend asks “What do you want to play with?”
- Behavior: The child says “ball”
- Reinforcement: The conversation continues, the child gets to play
Intraverbals are how everyday conversation works. Most social interactions are built on intraverbal exchanges.
From our experience at ABS: One of the most common patterns we see in newly enrolled children is what BCBAs call tact-rich, mand-poor, the child can label hundreds of objects but cannot use those same words to ask for what they want. This is the exact gap the VB approach is designed to address. Watching a child make their first true mand, choosing communication over a tantrum is one of the most rewarding moments in our work.
Why Mand Training Comes First in VB Programs?
Most VB-based programs prioritize mand training before other operants. This is not arbitrary, it is based on decades of research showing several practical benefits [6]:
- Mands give language immediate value. A child who learns “juice” as a mand gets juice. The reinforcement is direct, fast, and meaningful.
- Mands reduce challenging behavior. Many tantrums, aggression, and self-injury occur because a child cannot communicate what they want. Teaching the child to mand often reduces these behaviors dramatically.
- Mands build motivation to communicate. Once a child learns that words work, they become much more willing to engage with language teaching in general.
- Mand training often produces collateral gains. Research has shown that mand training can establish echoic and tact skills as side effects, even when those weren’t directly targeted [7].
For these reasons, your BCBA may spend the first several weeks or months of therapy focusing heavily on mand training before significantly expanding into other operants.
Wondering which skills your child would work on first?
What is The VB-MAPP? How Your Child's Skills Are Assessed?
The Verbal Behavior Milestones Assessment and Placement Program (VB-MAPP) is the most widely used assessment tool in modern VB-based ABA programs. It was developed by Dr. Mark L. Sundberg, BCBA-D, and published in its current second edition in 2014 [3].
The VB-MAPP measures 170 specific learning milestones across 16 skill areas, sequenced into three developmental levels:
Level | Developmental Range | Examples of Skills Assessed |
Level 1 | 0–18 months | Early mand skills, echoic responses, eye contact, motor imitation |
Level 2 | 18–30 months | Vocabulary expansion, simple intraverbals, basic listener skills |
Level 3 | 30–48 months | Conversation, advanced intraverbals, early academic skills |
Beyond milestones, the VB-MAPP also assesses:
- 24 barriers to learning: challenges that may slow language acquisition, such as prompt dependence, scrolling, or weak imitation
- Transition readiness: whether the child is ready to move to a less restrictive educational setting
The VB-MAPP is not a diagnostic tool. It does not diagnose autism, and it should not be used to determine eligibility for services. Its purpose is to give your child’s BCBA a clear picture of where to start teaching and how to measure progress. For more on assessments used in ABA, see our guide on Types of ABA Assessments.
What Does a VB Therapy Session Look Like?
A typical VB-based ABA session lasts 1 to 3 hours and is delivered by a Registered Behavior Technician (RBT) under the supervision of a Board Certified Behavior Analyst (BCBA). VB sessions often look very similar to NET or PRT sessions because they’re highly play-based and child-led, but with a deliberate focus on building specific verbal operants.
Here is what a real 90-minute session might look like for a 3-year-old child working on early mand and tact skills:
- Setting up the environment. The therapist arranges preferred items, favorite toys, snacks, bubbles visible but slightly out of reach. This creates natural motivation for the child to mand.
- Capturing motivation. The child reaches for the bubbles. The therapist holds them up and waits.
- Prompting a mand. The therapist says “Say bubbles” (an echoic prompt). The child says “bubbles.”
- Delivering natural reinforcement. The therapist immediately blows bubbles for the child to chase. This is the mand cycle.
- Layering in tacts. During play, the therapist points at the bubbles and says “Look! Bubbles!” modeling the tact function of the same word.
- Introducing simple intraverbals. During a snack break, the therapist asks “What do you want?” prompting the child to use “cookie” as an intraverbal response.
- Fading prompts. Over time, the therapist gradually removes the prompts so the child mands, tacts, and converses independently.
- Recording data. Each trial is tracked so the BCBA can see which operants are strengthening and where progress is slower.
The same session may also include time at a table for more structured DTT-style teaching of specific verbal targets, depending on the child’s current goals.
Is The VB Approach Evidence-Based?
Yes. The VB approach has a strong research foundation built up over several decades. Sundberg and Michael’s 2001 paper in Behavior Modification, “The benefits of Skinner’s analysis of verbal behavior for children with autism,” is one of the most cited works in the field and laid out the theoretical and practical case for VB-based teaching [2].
Beyond that foundational paper, the evidence base includes:
- Numerous peer-reviewed studies in the Journal of Applied Behavior Analysis and The Analysis of Verbal Behavior
- Research on how mand training produces collateral gains in echoic and other operants [7]
- Studies on how the VB-MAPP guides effective program design [3]
- Recognition by the American Academy of Pediatrics as part of evidence-based ABA therapy for autism [8]
That said, one important nuance: research strongly supports the VB approach as a framework for organizing language instruction within ABA. It is less of a standalone therapy and more of a way of structuring how language goals are written, taught, and measured. This is why VB principles are usually embedded inside broader ABA programs rather than offered as a separate service.
VB vs DTT vs NET vs PRT: How They Work Together
These four methods are often described as alternatives, but in practice, they are not in competition. A quality ABA program uses all of them, with the right blend determined by your child’s age, skills, and goals.
Feature | DTT | NET | PRT | VB Approach |
Primary focus | Specific behaviors | Generalization in real settings | Pivotal areas (motivation, etc.) | Functional language operants |
Setting | Table, structured | Wherever the child plays | Wherever the child plays | Both structured and natural |
Who leads | Therapist | Child’s interest | Child’s interest | Combination |
Reinforcer | Often arbitrary | Natural | Natural | Often natural |
Best at | Building foundational skills | Real-world generalization | Motivation + social communication | Building functional language |
Typically combined with | NET, VB | DTT, VB | DTT, NET | All three |
The VB approach is essentially the language layer that runs through the other methods. Your BCBA may use DTT to teach a child to label colors (tact training), NET to help the child request items during play (mand training), and PRT to encourage social initiations (intraverbal training in a social context). All of these use VB principles to organize what’s being taught.
For a complete decision guide comparing all four methods and specific recommendations by age and child profile, see our guide to Types of ABA Therapy Methods: DTT, NET, PRT, and VB Explained.
Ready to talk to a BCBA about your child?
Frequently Asked Questions About the VB Approach
Is the VB approach only for children with autism?
No. While the VB approach has been most widely researched and applied with children with autism, the underlying principles work for any individual with language delays, including children with intellectual disabilities, developmental delays, or apraxia of speech.
At what age can VB-based therapy start?
VB-based ABA therapy can start as early as 18 months. Many children begin VB programs during early intervention, which research consistently supports as the most effective window for language development. For more on starting ABA young, see our guide on ABA therapy for toddlers.
Can my child use sign language or AAC devices in a VB program?
Yes. The VB approach is not limited to spoken language. Sign language, picture exchange systems (PECS), and augmentative and alternative communication (AAC) devices can all serve as the behavior in a verbal operant. A child who signs “more” to request another bubble has performed a mand, just as much as a child who says “more” out loud.
Does my child need both VB-based ABA and speech therapy?
Many children benefit from both, since speech therapy and VB-based ABA address different aspects of communication. Your BCBA and Speech-Language Pathologist will coordinate to ensure the two programs reinforce each other rather than overlap. We discuss this further in our ABA vs speech therapy comparison.
Is the VB-MAPP the same as a diagnosis?
No. The VB-MAPP is an assessment of current language and learning skills used to plan a teaching program. It is not a diagnostic tool and cannot diagnose autism or any other condition. Diagnosis requires a separate evaluation by a qualified professional. See our guide on autism evaluations for more.
Is VB-based ABA covered by insurance?
Yes. The VB approach is part of standard ABA therapy and is included in insurance coverage from major carriers including Aetna, Cigna, UnitedHealthcare, Anthem BCBS, and state Medicaid programs in eligible states. See our ABA therapy insurance guide for New York for details on verifying your benefits.
Talk To a BCBA About VB-Based ABA For Your Child
The VB approach is not something you choose separately from ABA therapy, it is built into how a quality BCBA designs your child’s language goals. If you’d like to understand how VB principles would shape your child’s specific program, the starting point is a comprehensive assessment by a Board Certified Behavior Analyst. The Achievement Behavior Services team has supported families across New York, New Jersey, Connecticut, Georgia, and North Carolina since 2015 and would be glad to answer your questions.
References
[1] Skinner, B. F. (1957). Verbal Behavior. New York: Appleton-Century-Crofts.
https://psycnet.apa.org/PsycBOOKS/toc/11256
[2] Sundberg, M. L., & Michael, J. (2001). “The Benefits of Skinner’s Analysis of Verbal Behavior for Children with Autism.” Behavior Modification, 25(5), 698–724.
https://pubmed.ncbi.nlm.nih.gov/11573336/
[3] Sundberg, M. L. (2014). The Verbal Behavior Milestones Assessment and Placement Program: The VB-MAPP (2nd ed.). Concord, CA: AVB Press.
https://marksundberg.com/vb-mapp/
[4] Carbone, V. J., Sweeney-Kerwin, E. J., Attanasio, V., & Kasper, T. (2010). “Increasing the Vocal Responses of Children with Autism and Developmental Disabilities Using Manual Sign Mand Training and Prompt Delay.” Journal of Applied Behavior Analysis, 43(4), 705–709. https://pmc.ncbi.nlm.nih.gov/articles/PMC2998260/
[5] Cooper, J. O., Heron, T. E., & Heward, W. L. (2020). Applied Behavior Analysis (3rd ed.). Hoboken, NJ: Pearson Education.
https://www.pearson.com/en-us/subject-catalog/p/applied-behavior-analysis/P200000000905/9780137477210
[6] Drash, P. W., High, R. L., & Tudor, R. M. (1999). “Using Mand Training to Establish an Echoic Repertoire in Young Children with Autism.” The Analysis of Verbal Behavior, 16, 29–44. https://pubmed.ncbi.nlm.nih.gov/22477156/
[7] Marchese, N. V., Carr, J. E., LeBlanc, L. A., Rosati, T. C., & Conroy, S. A. (2012). “The Effects of the Question ‘What Is This?’ on Tact-Training Outcomes of Children with Autism.” Journal of Applied Behavior Analysis, 45(3), 539–547.
https://pubmed.ncbi.nlm.nih.gov/23060668/
[8] Hyman, S. L., Levy, S. E., Myers, S. M., & AAP Council on Children with Disabilities. (2020). “Identification, Evaluation, and Management of Children With Autism Spectrum Disorder.” Pediatrics, 145(1).
https://pubmed.ncbi.nlm.nih.gov/31843864/
