Pivotal Response Treatment (PRT) is a play-based, naturalistic form of ABA therapy developed by Drs. Robert and Lynn Kern Koegel. PRT targets four pivotal areas: motivation, responding to multiple cues, self-management, and social initiations, to produce widespread gains in communication.
If your child’s ABA program is heavy on play, follows your child’s lead, and uses their favorite toys as the rewards, you may already be seeing Pivotal Response Treatment in action. PRT is one of the most studied naturalistic ABA methods and is often combined with Discrete Trial Training (DTT) and Natural Environment Teaching (NET) to create a balanced therapy program.
This guide explains what PRT is, how it differs from other ABA methods, the four pivotal areas it targets, and what a session looks like in real life.
What is Pivotal Response Treatment in ABA?
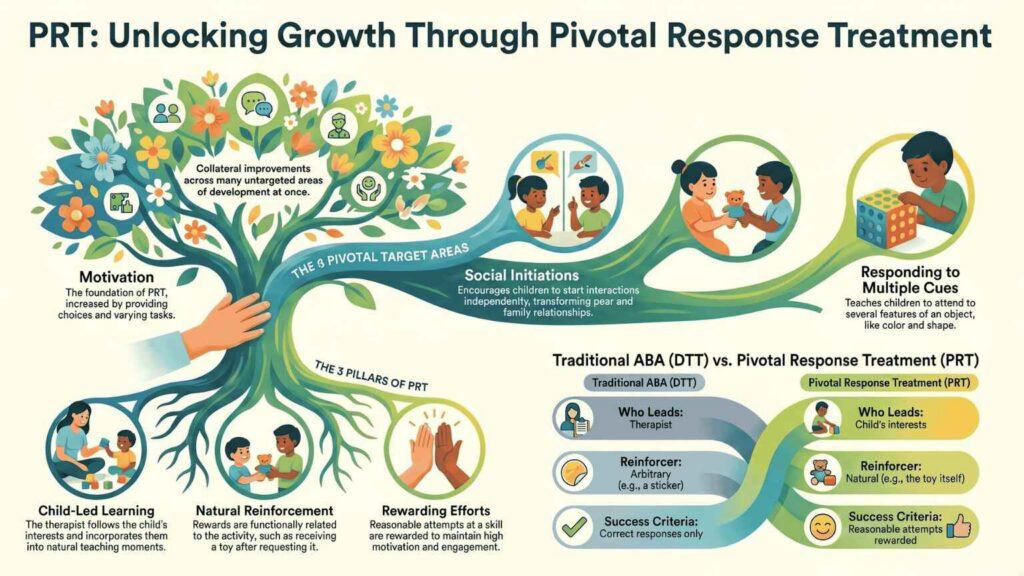
Pivotal Response Treatment is a naturalistic intervention derived from Applied Behavior Analysis that focuses on a small set of pivotal developmental skills rather than teaching individual behaviors one at a time. The core idea is that when you improve a pivotal skill such as motivation or social initiation, it produces collateral improvements across many other untargeted areas of development at once [1].
PRT was developed in the 1970s and 1980s by Dr. Robert L. Koegel and Dr. Lynn Kern Koegel, originally at the University of California, Santa Barbara, and now continued at the Stanford PRT Research and Training Program [2]. Over 200 peer-reviewed studies have been published on PRT in the past three decades, making it one of the most extensively researched naturalistic ABA approaches.
Three things define PRT:
- It targets pivotal skills, not individual behaviors. Instead of teaching a child to say 50 specific words one at a time, PRT teaches motivation to communicate, which then helps the child acquire many words.
- It is child-led. The therapist follows the child’s interests and incorporates them into teaching moments.
- It uses natural reinforcement. When a child requests a toy, the reward is that toy, not an unrelated treat or sticker.
PRT is not a separate therapy from ABA. It is one of several techniques used within Applied Behavior Analysis, and quality programs typically combine PRT with DTT and NET based on each child’s needs.
Looking for play-based ABA therapy for your child?
Fill in the form below to discuss how your child could start therapy quickly, without the stress:
How is PRT Different From Traditional ABA?
Traditional ABA, particularly DTT, often involves a therapist directing structured trials at a table with arbitrary rewards (such as a token or snack) for correct responses. PRT works very differently:
Feature | Traditional ABA / DTT | Pivotal Response Treatment (PRT) |
Focus | One specific behavior at a time | Pivotal skills that produce broad gains |
Who leads | The therapist | The child’s interests |
Setting | Often structured table or area | Wherever the child plays |
Reinforcer | Often arbitrary (token, treat) | Naturally related to the activity |
What earns the reward | Only correct responses | Reasonable attempts also rewarded |
Pacing | Therapist-controlled | Child-controlled |
A randomized clinical trial published in the Journal of Autism and Developmental Disorders in 2014 compared PRT with structured ABA in a school setting and found that PRT produced greater gains in social communication skills, including conversational initiations and pragmatic language use [3].
This does not mean PRT is “better” than DTT, they serve different purposes. DTT is excellent for building foundational, repeatable skills. PRT excels at expanding motivation, social communication, and generalization. Most effective programs use both.
What Are The 4 Pivotal Areas Targeted By PRT?
PRT focuses on four specific pivotal skills, chosen because improvement in any one of them tends to produce widespread improvements in many untargeted areas [4]:
1. Motivation
Motivation is the foundation of PRT. Many children with autism appear to disengage from learning not because they cannot learn, but because traditional teaching does not feel rewarding to them. PRT increases motivation by giving the child choice, varying tasks, and ensuring the reward is something the child actually wants.
2. Responding To Multiple Cues
Children with autism sometimes focus on a single feature of a complex situation for example, noticing only the color of an object while missing its shape or function. PRT teaches children to attend to multiple relevant features at once, which improves learning across nearly every context.
3. Self-Management
Self-management means the child can monitor and regulate their own behavior for example, recognizing when they need a break, completing a task without constant prompting, or transitioning between activities. Building self-management reduces the need for adult supervision and supports independence.
4. Social Initiations
This refers to the child starting social interactions on their own, asking a question, inviting a peer to play, commenting on something they notice. Social initiation is often a major gap for children with autism, and improving it transforms peer relationships, classroom participation, and family life.
The Motivation Strategies That Make PRT Work
Within the four pivotal areas, PRT uses a specific set of motivation strategies that have been refined through decades of research. Your child’s BCBA will use these throughout every session [5]:
- Child choice: The child picks which toy, activity, or topic to work on. This dramatically increases engagement.
- Task variation: Sessions mix easier mastered tasks with newer, harder ones. This prevents frustration and keeps motivation high.
- Rewarding attempts: A reasonable attempt at the target skill earns the reward, not only perfect responses. This is one of the biggest differences from traditional ABA.
- Natural reinforcement: The reward is functionally connected to the response. Asking for a ball gets the ball. Asking for a turn at the swing gets the turn at the swing.
- Turn-taking: The therapist takes turns with the child to keep social engagement active throughout the session.
From our experience at ABS: We often introduce PRT-based teaching for children who resist structured table-work or who have strong, identifiable interests we can leverage. The motivational shift, letting the child pick the activity and rewarding them with that exact thing, frequently produces breakthrough engagement in children who had previously seemed disengaged from therapy. PRT is not a replacement for structured teaching, but it can be the bridge that makes structured teaching possible.
Has traditional ABA felt like a struggle for your child?
What Does a PRT Session Look Like?
A typical PRT session lasts 1 to 3 hours and takes place in your home, at a therapy center, or in a community setting such as a park or playground. The therapist is usually a Registered Behavior Technician (RBT) working under the supervision of a Board Certified Behavior Analyst (BCBA).
Here is what a real PRT session might look like for a 4-year-old child working on requesting and conversation skills:
- The therapist arrives with a few options based on the child’s known interests, say, a train set, a bubble machine, and a small bin of dinosaur figurines.
- The child picks one (child choice) train.
- The therapist holds two trains and waits, offering an antecedent like “Which one?” (motivation through choice).
- The child reaches and says “blue” (a reasonable attempt, even if not a full sentence).
- The therapist gives the blue train immediately and joins the play (natural reinforcement + turn-taking).
- A few minutes in, the therapist mixes in a known-easy task “Show me the train tracks” to maintain success momentum, then loops back to harder targets.
- The therapist embeds opportunities to practice multiple cues “Get the small red train” (color + size + object).
- Throughout, the therapist records data on initiations, attempts, and correct responses for the BCBA to review.
To an observing parent, much of this looks like ordinary play. That is the point, PRT is designed to make learning feel natural so the child stays engaged and the skills transfer into real life [6].
What Skills Does PRT Help Develop?
Research on PRT consistently shows improvements in three core areas across the majority of children who receive it [7][8]:
- Communication and language: PRT excels at increasing functional verbal utterances, vocabulary, and conversational ability. Stanford’s PRT research program has reported that 85–90% of children with autism who begin PRT before age 5 develop verbal communication as their primary mode of expression [2].
- Play skills: Toy play, symbolic play, and peer play all improve significantly with PRT.
- Social initiation and engagement: Children show increased eye contact, joint attention, and self-initiated social bidding.
For some children, PRT also produces collateral reductions in challenging behaviors and improvements in mood and affect, although the evidence base for these outcomes is less conclusive [7]. PRT is not designed to address every aspect of autism, and most quality programs combine PRT with other ABA methods to cover skills that PRT alone does not target as effectively.
Is PRT Evidence-Based? What The Research Shows
Yes. PRT is one of the most extensively researched naturalistic ABA interventions, with over 200 peer-reviewed studies published since the 1970s [6]. Major evidence highlights include:
- A 2015 consensus paper in the Journal of Autism and Developmental Disorders classified PRT as a research-supported Naturalistic Developmental Behavioral Intervention (NDBI) [4].
- A 2014 randomized clinical trial found PRT more effective than structured ABA for improving social communication in school-age children with autism [3].
- Brain imaging research has documented changes in brain activity associated with social engagement after PRT intervention, suggesting the gains are not just behavioral but neurological.
- The American Academy of Pediatrics recognizes naturalistic, behavior-analytic interventions as evidence-based components of autism care [9].
There is one important nuance worth knowing as a parent: a systematic review found strong evidence for PRT’s effects on language, communication, and play, but less conclusive evidence on broader outcomes such as cognitive functioning or autism symptom severity [7]. This is not unusual for any single therapy method, it is why most quality ABA programs combine multiple approaches.
PRT vs DTT vs NET: How The Three Methods Compare
PRT, DTT, and NET are often discussed together because most modern ABA programs blend all three. Here’s the quick comparison:
Feature | DTT | NET | PRT |
Setting | Table, structured | Floor, kitchen, playground | Wherever the child plays |
Who leads | Therapist | Child’s interest | Child’s interest |
Focus | Specific behaviors | General skill generalization | 4 pivotal areas |
Reinforcer | Often arbitrary | Natural | Natural |
Best for | Foundational skill building | Real-life skill generalization | Motivation + social communication |
The right blend depends on your child’s age, current skills, and goals. A 2-year-old just starting therapy may benefit from heavy PRT and NET to build motivation, with DTT introduced gradually. A 7-year-old with strong communication but weak academic skills may benefit from more DTT focused on specific learning targets, with PRT used to support social development.
For a complete decision guide comparing all four major ABA methods DTT, NET, PRT, and VB and which blend likely fits your child best, see our guide to Types of ABA Therapy Methods: DTT, NET, PRT, and VB Explained.
Ready to find the right ABA program for your child?
Frequently Asked Questions About PRT
Is PRT only for children with autism?
PRT was developed for autism and has the strongest evidence base in that population, but the underlying motivational strategies are also used in early intervention for other developmental delays. If you have questions about whether PRT fits your child’s specific diagnosis, your BCBA can advise during the ABA assessment.
At what age can PRT start?
PRT has been studied in children as young as 2 and as old as 16. The research base is strongest for ages 2 to 7, when language and social skills are developing most rapidly. Beginning PRT before age 5 produces particularly strong outcomes for verbal communication development [2]. Our early intervention program uses PRT-based teaching extensively for toddlers and preschoolers.
Can I do PRT at home with my child?
Yes and you should. Parent involvement is one of PRT’s defining features, and a substantial body of research supports parent-mediated PRT as an effective intervention model. Most quality ABA programs include structured parent training so families can use PRT strategies during everyday routines such as snack time, bath time, and play [5].
How long does PRT take to show results?
Most children show measurable changes within 8 to 12 weeks of consistent PRT-based intervention, though the timeline varies based on intensity, the child’s starting skills, and parent involvement at home.
Is PRT covered by insurance?
Yes. PRT is considered part of standard ABA therapy and is included in coverage from most major insurance carriers including Aetna, Cigna, UnitedHealthcare, Anthem BCBS, and state Medicaid programs in eligible states. See our ABA therapy insurance guide for New York for details on verifying your benefits.
Will my child still need DTT and NET?
Most likely yes. PRT excels at motivation and social communication, but DTT is often better for building specific foundational skills (letter recognition, math facts, precise imitation), and NET is excellent for generalizing skills across real-world settings. A well-designed program uses the right blend for each child.
Talk To A BCBA About Whether PRT is Right For Your Child
Choosing the right blend of ABA methods is not something to figure out alone and your child’s specific needs may call for a unique combination of PRT, DTT, NET, and other techniques. The best way to know is through a comprehensive assessment by a Board Certified Behavior Analyst. Our team has supported families across New York, New Jersey, Connecticut, Georgia, and North Carolina since 2015 and would be glad to answer your questions.
References
[1] Koegel, R. L., & Koegel, L. K. (2006). Pivotal Response Treatments for Autism: Communication, Social, and Academic Development. Baltimore: Paul H. Brookes Publishing.
https://brookespublishing.com/wp-content/uploads/2020/05/Koegel-2e_excerpt.pdf
[2] Stanford PRT Research and Training Program, Stanford University School of Medicine. “Pivotal Response Treatment.”
https://med.stanford.edu/autismcenter/prt.html
[3] Mohammadzaheri, F., Koegel, L. K., Rezaee, M., & Rafiee, S. M. (2014). “A Randomized Clinical Trial Comparison Between Pivotal Response Treatment (PRT) and Structured Applied Behavior Analysis (ABA) Intervention for Children with Autism.” Journal of Autism and Developmental Disorders, 44(11), 2769–2777.
https://pmc.ncbi.nlm.nih.gov/articles/PMC4194254/
[4] Schreibman, L., Dawson, G., Stahmer, A. C., Landa, R., Rogers, S. J., McGee, G. G., et al. (2015). “Naturalistic Developmental Behavioral Interventions: Empirically Validated Treatments for Autism Spectrum Disorder.” Journal of Autism and Developmental Disorders, 45(8), 2411–2428. https://pubmed.ncbi.nlm.nih.gov/25737021/
[5] Koegel, R. L., Schreibman, L., Good, A., Cerniglia, L., Murphy, C., & Koegel, L. K. (1989). “How to Teach Pivotal Behaviors to Children with Autism: A Training Manual.” University of California, Santa Barbara.
https://neurosciences.ucsd.edu/centers-programs/autism/_files/about-autism/peer-training-manual-2007.pdf
[6] Yale Medicine. “Pivotal Response Treatment Fact Sheet.” https://www.yalemedicine.org/conditions/pivotal-response-treatment
[7] Verschuur, R., Didden, R., Lang, R., Sigafoos, J., & Huskens, B. (2014). “Pivotal Response Treatment for Children with Autism Spectrum Disorders: A Systematic Review.” Review Journal of Autism and Developmental Disorders, 1(1), 34–61.
https://link.springer.com/article/10.1007/s40489-013-0008-z
[8] Bozkus-Genc, G., & Yucesoy-Ozkan, S. (2016). “Meta-Analysis of Pivotal Response Training for Children with Autism Spectrum Disorder.” Education and Training in Autism and Developmental Disabilities, 51(1), 13–26.
https://journals.sagepub.com/doi/10.1177/215416471605100103
[9] Hyman, S. L., Levy, S. E., Myers, S. M., & AAP Council on Children with Disabilities. (2020). “Identification, Evaluation, and Management of Children With Autism Spectrum Disorder.” Pediatrics, 145(1).
https://publications.aap.org/pediatrics/article/145/1/e20193447/36917/Identification-Evaluation-and-Management-of
