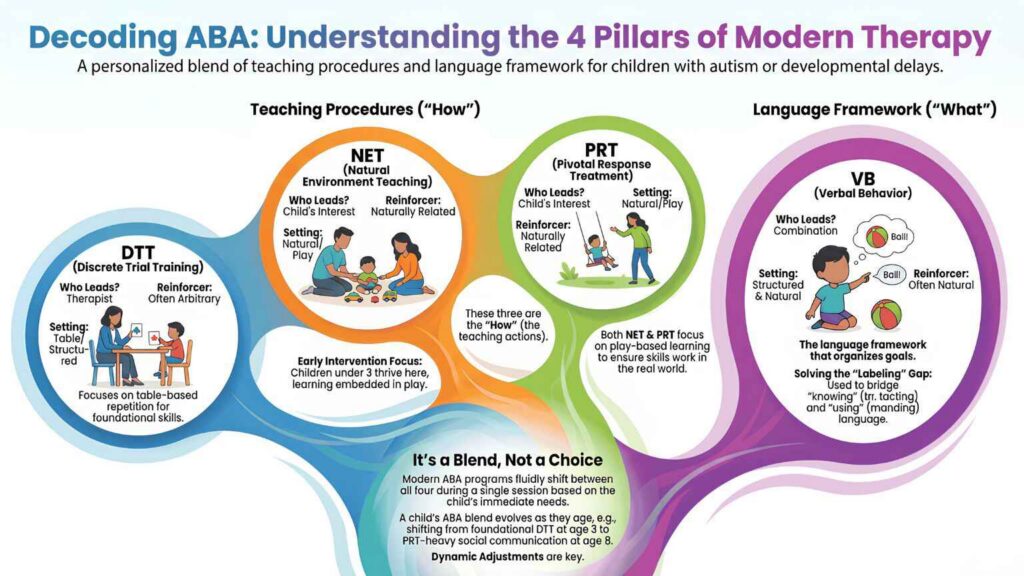
There are four main types of ABA therapy methods used today: Discrete Trial Training (DTT), Natural Environment Teaching (NET), Pivotal Response Treatment (PRT), and the Verbal Behavior (VB) approach. DTT, NET, and PRT are teaching procedures, while VB is a framework for organizing language goals. Most quality ABA programs combine all four.
If you’re researching ABA therapy for your child, you’ve probably come across confusing names like DTT, NET, PRT, and VB. Each one is described as a different ABA method, and most blogs present them as if you need to choose between them.
The truth is more nuanced and once you understand it, the choice gets much easier. This guide explains each of the four major ABA methods in plain language, shows you how they actually work together, and gives you specific decision criteria for which blend is likely to fit your child best.
What Are the Main Types of ABA Therapy Methods?
ABA therapy is not a single technique. It’s a broad framework that includes multiple teaching procedures, each with its own strengths. The four most widely used methods in modern ABA practice are:
- Discrete Trial Training (DTT): structured, table-based teaching with clear trials and rewards
- Natural Environment Teaching (NET): child-led, play-based teaching that happens during everyday activities
- Pivotal Response Treatment (PRT): naturalistic teaching that targets four pivotal developmental skills
- The Verbal Behavior (VB) Approach: a framework for teaching language by its function
Each method is supported by decades of peer-reviewed research, and each is recognized by the American Academy of Pediatrics as part of evidence-based ABA care [1]. The differences between them lie in how a session is structured, who leads the learning, and what the reward looks like.
For an in-depth look at Applied Behavior Analysis as a whole, see our full guide.
The 4 ABA Methods At a Glance
Here is how the four major methods compare across the criteria that matter most to parents:
Feature | DTT | NET | PRT | VB Approach |
Type of method | Teaching procedure | Teaching procedure | Teaching procedure | Language framework |
Setting | Table, structured area | Wherever the child plays | Wherever the child plays | Both structured and natural |
Who leads | Therapist | Child’s interest | Child’s interest | Combination |
Pace | Therapist-controlled | Child-controlled | Child-controlled | Varies |
Reinforcer | Often arbitrary (token, snack) | Naturally related to task | Naturally related to task | Often natural |
What earns the reward | Correct responses | Correct attempts | Reasonable attempts | Functional use of language |
Best for | Foundational skills, repetition | Generalization in real settings | Motivation, social communication | Functional language across operants |
Typical age range | 2 to teens | 2 to 7 (strongest evidence) | 2 to 16 | 18 months and up |
The most important row in this table is the first one: type of method. Three of these are teaching procedures, but VB is a language framework. That distinction changes how you think about choosing.
Ready to talk to a BCBA about the right ABA blend for your child?
Our BCBAs design personalized ABA programs that combine DTT, NET, PRT, and VB principles based on what your child actually needs.
Discrete Trial Training (DTT) - When It's the Right Fit
Discrete Trial Training is the most structured of the four methods. The therapist directs short, repeatable teaching trials at a table or designated workspace, each following a clear pattern: instruction, child’s response, reward.
DTT excels at teaching skills that benefit from many repetitions in a controlled setting, things like letter identification, number sequences, naming colors, motor imitation, and self-help routines.
When DTT is The Right Primary Method
Consider DTT-heavy programming if your child:
- Is just beginning to learn new skills and needs predictable, repetitive teaching
- Responds well to structured environments
- Needs strong foundational skills before moving to more naturalistic teaching
- Has goals that require precise, measurable responses (such as academic readiness)
When DTT Alone is Not Enough
DTT is less effective for skills that depend on spontaneity, motivation, or social context. A child who can name 100 objects at a table but cannot request any of them in real life is showing the classic limitation of DTT used alone. This is why modern programs almost never use DTT as the only method.
For the full explanation of how DTT works, see our Discrete Trial Training guide.
Natural Environment Teaching (NET) - When it's The Right Fit
Natural Environment Teaching is the play-based counterpart to DTT. The therapist follows the child’s interests during everyday activities, floor play, snack time, the playground and turns those moments into teaching opportunities. The reward is always naturally connected to the task: a child who requests a bubble gets the bubble blown.
NET excels at helping children use skills in real-life contexts (generalization), build spontaneous communication, and stay engaged during long therapy sessions.
When NET is The Right Primary Method
Consider NET-heavy programming if your child:
- Resists structured table work or becomes frustrated with sit-down teaching
- Has the basic skill set but doesn’t use skills outside the therapy room (a generalization gap)
- Is in early intervention years (ages 2 to 7) when naturalistic teaching produces strongest outcomes
- Has strong personal interests that can be leveraged for motivation
When NET Alone is Not Enough
NET is less effective at building completely new foundational skills, because the unpredictability of real environments makes structured repetition difficult. Children who need to learn letter sounds, math facts, or precise motor imitation usually benefit from DTT support alongside NET.
For the full explanation of how NET works, see our Natural Environment Teaching guide.
Pivotal Response Treatment (PRT) - When it's The Right Fit
Pivotal Response Treatment is a naturalistic method developed by Drs. Robert and Lynn Kern Koegel that focuses on four pivotal developmental areas: motivation, responding to multiple cues, self-management, and social initiations. Improving these pivotal skills produces widespread improvements in many untargeted areas at once.
PRT excels at building motivation, expanding social communication, and producing collateral gains across the child’s overall development.
When PRT is The Right Primary Method
Consider PRT-heavy programming if your child:
- Has seemed disengaged or unmotivated during previous therapy attempts
- Has strong identifiable interests (specific toys, characters, topics) that can power motivation
- Needs to build conversational and social initiation skills
- Would benefit from teaching that feels indistinguishable from play
When PRT Alone is Not Enough
PRT excels at language and social communication, but the evidence base is less conclusive for outcomes like cognitive functioning or autism symptom severity [2]. Children with significant cognitive or academic goals typically benefit from DTT alongside PRT.
For the full explanation of how PRT works, see our Pivotal Response Treatment guide.
The Verbal Behavior (VB) Approach and Why It's a Framework, Not a Competing Method?
This is the most important section of this guide, because it resolves the single biggest confusion parents have when choosing between ABA methods.
The VB approach is not a teaching procedure like DTT, NET, or PRT. It is a framework for organizing how language is taught across all of those methods.
The VB approach, based on B.F. Skinner’s analysis of verbal behavior, says that language has different functions requesting (mand), labeling (tact), repeating (echoic), and conversing (intraverbal) and each function needs to be taught separately. [4] A child who learns the word “cookie” as a label (tact) cannot automatically use that word to request a cookie (mand). Each verbal operant is its own skill.
What this means in practice: your child’s BCBA will use VB principles to decide WHAT to teach, then use DTT, NET, or PRT to decide HOW to teach it. The methods are not in competition, they operate at different levels.
For example, a single language goal “child will request preferred items” might be taught using:
- DTT for the structured trials that build the basic mand response
- NET for practicing the mand during real-life play with preferred toys
- PRT for using natural reinforcement to deepen motivation to mand
- VB principles to track that the child can mand across multiple operants and contexts
For the full explanation of how VB works, see our Verbal Behavior approach guide.
When The VB Framework Matters Most
VB principles should drive your child’s program if:
- Communication is the primary therapy goal
- Your child shows the “tact-rich, mand-poor” pattern (can label things but can’t request them)
- Your child uses sign language, picture exchange, or AAC devices in addition to (or instead of) spoken language
- You want clear measurement of which functional language skills are developing
How Most Quality ABA Programs Combine These Methods
Modern ABA programs do not pick one method. They blend all four based on the child’s age, current skills, and goals. Here is what a typical balanced program might look like across a 2-hour session for a 4-year-old:
Time | Activity | Primary Method | What’s Being Taught |
0:00–0:20 | Table-based DTT | DTT with VB framework | New vocabulary as tacts |
0:20–0:40 | Floor play with preferred toys | NET + PRT | Same vocabulary as mands |
0:40–1:00 | Pretend play / role play | PRT + VB | Intraverbal exchanges in social context |
1:00–1:15 | Snack time | NET with VB framework | Mand training around natural motivators |
1:15–1:30 | Outdoor or sensory play | PRT | Self-management and turn-taking |
1:30–1:50 | Structured table work | DTT | Pre-academic skills, motor imitation |
1:50–2:00 | Parent training / data review | All methods | Caregiver coaching for home carryover |
From our experience at ABS: The best ABA programs we’ve seen and the ones we design never look like a single method being applied for the full session. They look like a flowing blend where the therapist constantly shifts technique based on the child’s energy, focus, and current goal. A skilled BCBA spends as much time deciding which method to use when as they do designing what to teach.
Which ABA Method is Right For My Child? A Decision Guide
Every child is different, but certain patterns hold true often enough to give general guidance. Here is what we typically recommend at Achievement Behavior Services based on the child’s age and presentation:
1. Children Under 3, Pre-Verbal or Minimally Verbal
Recommended blend: NET-heavy with PRT, mand training prioritized using VB framework, DTT introduced gradually.
These children benefit most from naturalistic, motivation-based teaching. Pulling a 2-year-old to a table for long stretches typically backfires, they need learning embedded in play and connected to their natural interests. Early mand training transforms their ability to communicate without resorting to behavior. For more on starting therapy young, see our early intervention guide and ABA therapy for toddlers.
2. Children Ages 3 to 5 With Emerging Language
Recommended blend: Balanced DTT and NET, with PRT for social goals, organized through the VB framework.
This is the classic early intervention window. Foundational skills can now be built efficiently through structured DTT trials, while NET and PRT ensure those skills generalize to real-life use. The VB framework keeps language goals organized across all four operants.
3. Children Ages 6 to 12 With Established Language But Social or Academic Gaps
Recommended blend: PRT-heavy for social communication, DTT for specific academic targets, NET for community generalization.
At this age, motivation often becomes a bigger factor than basic skill acquisition. PRT excels at engaging school-age children, while DTT remains valuable for closing specific academic gaps. Generalization across school, home, and community settings becomes a major focus.
4. Children With Strong Receptive Skills But Limited Expressive Language
Recommended blend: Heavily VB-driven, with mand training prioritized above all else, using whichever teaching procedure (DTT, NET, or PRT) keeps the child engaged.
This profile, understanding language but struggling to use it, is one of the clearest indications that VB principles should drive the program. Identifying which operants are weak and building them systematically often produces dramatic communication gains.
5. Children Who Have Resisted Structured Therapy in The Past
Recommended blend: PRT and NET first, with DTT introduced only after motivation is established. VB framework used throughout.
For these children, leading with structured table work usually fails. Building motivation and engagement through PRT and NET makes structured teaching possible later, often within weeks rather than months.
6. Children Who Can Label Many Things But Rarely Use Language Functionally
Recommended blend: Strong VB focus with heavy mand training. DTT for new vocabulary, NET for practicing functional use in real settings.
This is the classic tact-rich, mand-poor pattern. The solution is rarely “more vocabulary”, it’s teaching the child that the words they already know have power when used as mands.
Did you recognize your child in one of those profiles?
Common Questions Parents Ask About Choosing An ABA Method
Do I have to choose one method?
No. Most quality ABA programs combine all four. The question isn’t which one but what blend and that decision belongs to a Board Certified Behavior Analyst based on your child’s specific assessment.
Can I ask my BCBA which methods they use?
Yes, and you should. A good BCBA will be able to explain not only which methods they use, but why they’re using each one for your child specifically. If a provider tells you they “only use DTT” or “don’t use PRT,” that’s a sign their program lacks the flexibility quality care requires.
How does my BCBA decide the blend?
Through a comprehensive ABA assessment, which includes tools like the VB-MAPP, observation of your child in different settings, and conversations with you about your child’s preferences, motivators, and family routines.
Will my child’s program change over time?
Yes. The right blend at age 3 is usually very different from the right blend at age 6 or 10. Your BCBA should be regularly reassessing and adjusting the program as your child’s skills grow.
Are all four methods covered by insurance?
Yes. All four are considered standard parts of ABA therapy and are covered by major insurance carriers including Aetna, Cigna, UnitedHealthcare, Anthem BCBS, and state Medicaid programs in eligible states. See our ABA therapy insurance guide for New York for details on verifying benefits.
Is one method more evidence-based than the others?
All four have strong research support. The Lovaas studies from the 1980s established DTT-based ABA’s evidence base, Hart and Risley’s work established NET’s foundation in the 1970s, the Koegels’ research has supported PRT for over 30 years, and Skinner’s analysis combined with decades of subsequent research supports the VB framework. The American Academy of Pediatrics recognizes all of these as components of evidence-based autism care [1].
Can I do any of these at home as a parent?
Yes, especially NET and PRT principles, and to some extent VB-based mand training. Most quality ABA programs include parent training so you can use the same techniques at home during everyday routines. The best results come from coordinated effort between the BCBA team and the family.
Talk To a BCBA About The Right ABA Blend For Your Child
Choosing between ABA methods isn’t really a choice between methods, it’s a choice of who you trust to design your child’s blend. A skilled Board Certified Behavior Analyst spends their career learning how to combine DTT, NET, PRT, and VB principles into a program that fits each child specifically.
Our team at Achievement Behavior Services has been designing personalized ABA programs across New York, New Jersey, Connecticut, Georgia, and North Carolina since 2015. Every program starts with a comprehensive BCBA assessment, most fully covered by insurance and is built around your child’s specific strengths, needs, and goals.
Ready to find the right ABA blend for your child?
References
[1] Hyman, S. L., Levy, S. E., Myers, S. M., & AAP Council on Children with Disabilities. (2020). “Identification, Evaluation, and Management of Children With Autism Spectrum Disorder.” Pediatrics, 145(1).
https://publications.aap.org/pediatrics/article/145/1/e20193447/36917/Identification-Evaluation-and-Management-of
[2] Verschuur, R., Didden, R., Lang, R., Sigafoos, J., & Huskens, B. (2014). “Pivotal Response Treatment for Children with Autism Spectrum Disorders: A Systematic Review.” Review Journal of Autism and Developmental Disorders, 1(1), 34–61.
https://link.springer.com/article/10.1007/s40489-013-0008-z
[3] Schreibman, L., Dawson, G., Stahmer, A. C., Landa, R., Rogers, S. J., McGee, G. G., et al. (2015). “Naturalistic Developmental Behavioral Interventions: Empirically Validated Treatments for Autism Spectrum Disorder.” Journal of Autism and Developmental Disorders, 45(8), 2411–2428.
https://pubmed.ncbi.nlm.nih.gov/25737021/
[4] Sundberg, M. L., & Michael, J. (2001). “The Benefits of Skinner’s Analysis of Verbal Behavior for Children with Autism.” Behavior Modification, 25(5), 698–724.
https://pubmed.ncbi.nlm.nih.gov/11573336/
[5] Lovaas, O. I. (1987). “Behavioral Treatment and Normal Educational and Intellectual Functioning in Young Autistic Children.” Journal of Consulting and Clinical Psychology, 55(1), 3–9.
https://pubmed.ncbi.nlm.nih.gov/3571656/
[6] Hart, B., & Risley, T. R. (1975). “Incidental Teaching of Language in the Preschool.” Journal of Applied Behavior Analysis, 8(4), 411–420.
https://pmc.ncbi.nlm.nih.gov/articles/PMC1311874/
[7] Mohammadzaheri, F., Koegel, L. K., Rezaee, M., & Rafiee, S. M. (2014). “A Randomized Clinical Trial Comparison Between Pivotal Response Treatment (PRT) and Structured Applied Behavior Analysis (ABA) Intervention for Children with Autism.” Journal of Autism and Developmental Disorders, 44(11), 2769–2777.
https://pmc.ncbi.nlm.nih.gov/articles/PMC4194254/
[8] Cooper, J. O., Heron, T. E., & Heward, W. L. (2020). Applied Behavior Analysis (3rd ed.). Hoboken, NJ: Pearson Education.
https://api.pageplace.de/preview/DT0400.9781292341057_A39573391/preview-9781292341057_A39573391.pdf
